【Hysteroscope】High-frequency Electrosurgical Unit Cutting Method
Release time: 06 Apr 2021 Author:Shrek
Indications for hysteroscopic surgery:
① Abnormal uterine bleeding. ②Endometrial polyps. ③Uterine fibroids that affect the shape of the uterine cavity. ④ Uterine adhesions. ⑤ Uterine malformation. ⑥ Foreign bodies in the uterine cavity. ⑦ Uterine cavity lesions related to pregnancy. ⑧ Abnormal endometrial hyperplasia. ⑨ Foreign body in the vagina of young girls.
Relative contraindications of hysteroscopic surgery:
① Body temperature>37.5℃. ② Active uterine bleeding and severe anemia. ③ Acute or subacute inflammation of the genital tract or pelvis. ④ Uterine perforation occurred recently. ⑤ The uterine cavity is too narrow or the cervical canal is narrow, hard, and difficult to expand. ⑥ Invasive cervical cancer and genital tuberculosis have not been treated for tuberculosis. ⑦Severe medical and surgical complications cannot tolerate surgical operations.
Basic requirements for hysteroscopic surgery:
①In the non-head-down lithotomy position, clamp the anterior lip of the cervix with cervical clamps, use the probe to detect the depth and direction of the uterine cavity, and dilate the cervix to 10-12 size with the cervical dilation rod. ②Using 5% dextrose solution or normal saline to dilate the uterus, first empty the air between the lens sheath and the optical lens tube, slowly insert the hysteroscope, turn on the light source, and inject the uterine dilatation fluid, the uterine pressure is 80-100mmHg or less than the average patient Arterial pressure, after the uterine cavity is filled, the visual field is bright, and the endoscope can be rotated and comprehensively observed in sequence. ③Check the fundus of the uterus and the front, back, left and right walls of the uterine cavity first, and then check the uterine horns and fallopian tube openings. Pay attention to the shape of the uterine cavity, whether there is abnormal endometrial or space-occupying lesions. ④Finally, carefully inspect the internal cervix and cervical canal while slowly pushing out the hysteroscope.
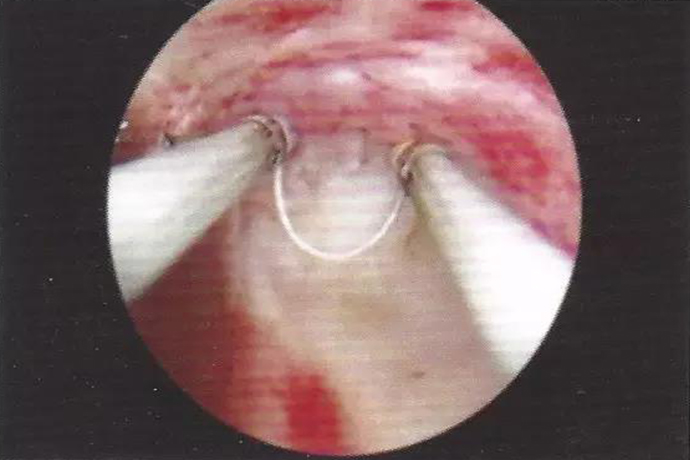
Anterograde resection
The hysteroscope high-frequency electrosurgical unit resection anterograde cutting method is a hysteroscope single-stage or bipolar ring electrode cutting from far and near anterograde to cut out long strips of tissue. This technology can clearly observe the movement process of the electric resection ring from far to near under the hysteroscope, avoiding the wrong cutting of adjacent tissues, and can repeat the operation to remove a large amount of tissue. It is endometrial resection, endometrial polypectomy, uterine muscle tumor resection, uterine mediastinum resection and other operations are the longest cutting methods used.
The specific operation method is:
(1) First, place the hysteroscope on the surface of the tissue to be cut to expose the surgical field of view.
(2) Push the ring electrode out of the sheath and extend it far away, and place it on the surface of the distal end of the tissue to be cut
(3) The foot switch is energized, and the electric cutting ring is appropriately cut into the tissue to an appropriate depth, and the hysteroscope is slowly pulled back with the sheath at the same time
(4) Pull back the hysteroscope with the sheath according to the requirements of the depth or length of the resection, and make parallel cuts far and near to reach the edge of the tissue to be cut.
(5) Pull back the ring electrode slowly to recover it into the sheath and cut off the tissue. Release the pedal, the power on stops, and the cutting ends.
Retrograde resection
The cutting direction of hysteroscopic high-frequency electrosurgical unit retrograde resection is opposite to that of antegrade resection, which uses ring electrodes to cut from near to far. However, the direction, distance and speed of the ring point pole moving far away during cutting cannot be clearly observed under the hysteroscope, and the operation is not easy to control. It is easy to push the ring electrode into the uterine wall and cause damage and even cause perforation. In view of the difficulty of this method, when there are more tissues to be removed and the distant boundary cannot be seen clearly; when the lower boundary of the tissue to be removed is floating and it is difficult to perform antegrade resection; or when there are some wounds on the wound after antegrade resection. The residual tissue is connected to the wound surface and flutters. If it is difficult to perform anterograde resection, it should be performed by an experienced doctor.
The specific operation method is:
(1) First, place the hysteroscope on the surface of the tissue to be cut to expose the surgical field.
(2) Push the ring electrode out of the sheath and place it on the surface of the proximal end of the tissue to be cut.
(3) Step on the electric resection pedal to energize, push the ring electrode forward to cut into the tissue to an appropriate depth, push it backwards for a short distance, and cut it off when it reaches the distal edge of the tissue to be removed.
Transverse resection
Hysteroscopic high-frequency electric transverse resection is to cut the ring electrode from left to right, or from right to left. During the resection, the movement of the electric resection ring is mainly based on the appropriate lateral movement of the sheath. This method is suitable for removing the tissue at the bottom of the uterus and the uterine septum.
Vertical excision
The high-frequency electric vertical resection method of hysteroscope is to cut the ring electrode vertically from top to bottom. When cutting, the movement of the electric resection ring is small, and the main purpose of the hysteroscope sheath is to move up and down properly. This method is suitable for the removal of larger fibroids.
① Abnormal uterine bleeding. ②Endometrial polyps. ③Uterine fibroids that affect the shape of the uterine cavity. ④ Uterine adhesions. ⑤ Uterine malformation. ⑥ Foreign bodies in the uterine cavity. ⑦ Uterine cavity lesions related to pregnancy. ⑧ Abnormal endometrial hyperplasia. ⑨ Foreign body in the vagina of young girls.
Relative contraindications of hysteroscopic surgery:
① Body temperature>37.5℃. ② Active uterine bleeding and severe anemia. ③ Acute or subacute inflammation of the genital tract or pelvis. ④ Uterine perforation occurred recently. ⑤ The uterine cavity is too narrow or the cervical canal is narrow, hard, and difficult to expand. ⑥ Invasive cervical cancer and genital tuberculosis have not been treated for tuberculosis. ⑦Severe medical and surgical complications cannot tolerate surgical operations.
Basic requirements for hysteroscopic surgery:
①In the non-head-down lithotomy position, clamp the anterior lip of the cervix with cervical clamps, use the probe to detect the depth and direction of the uterine cavity, and dilate the cervix to 10-12 size with the cervical dilation rod. ②Using 5% dextrose solution or normal saline to dilate the uterus, first empty the air between the lens sheath and the optical lens tube, slowly insert the hysteroscope, turn on the light source, and inject the uterine dilatation fluid, the uterine pressure is 80-100mmHg or less than the average patient Arterial pressure, after the uterine cavity is filled, the visual field is bright, and the endoscope can be rotated and comprehensively observed in sequence. ③Check the fundus of the uterus and the front, back, left and right walls of the uterine cavity first, and then check the uterine horns and fallopian tube openings. Pay attention to the shape of the uterine cavity, whether there is abnormal endometrial or space-occupying lesions. ④Finally, carefully inspect the internal cervix and cervical canal while slowly pushing out the hysteroscope.
Anterograde resection
The hysteroscope high-frequency electrosurgical unit resection anterograde cutting method is a hysteroscope single-stage or bipolar ring electrode cutting from far and near anterograde to cut out long strips of tissue. This technology can clearly observe the movement process of the electric resection ring from far to near under the hysteroscope, avoiding the wrong cutting of adjacent tissues, and can repeat the operation to remove a large amount of tissue. It is endometrial resection, endometrial polypectomy, uterine muscle tumor resection, uterine mediastinum resection and other operations are the longest cutting methods used.
The specific operation method is:
(1) First, place the hysteroscope on the surface of the tissue to be cut to expose the surgical field of view.
(2) Push the ring electrode out of the sheath and extend it far away, and place it on the surface of the distal end of the tissue to be cut
(3) The foot switch is energized, and the electric cutting ring is appropriately cut into the tissue to an appropriate depth, and the hysteroscope is slowly pulled back with the sheath at the same time
(4) Pull back the hysteroscope with the sheath according to the requirements of the depth or length of the resection, and make parallel cuts far and near to reach the edge of the tissue to be cut.
(5) Pull back the ring electrode slowly to recover it into the sheath and cut off the tissue. Release the pedal, the power on stops, and the cutting ends.
Retrograde resection
The cutting direction of hysteroscopic high-frequency electrosurgical unit retrograde resection is opposite to that of antegrade resection, which uses ring electrodes to cut from near to far. However, the direction, distance and speed of the ring point pole moving far away during cutting cannot be clearly observed under the hysteroscope, and the operation is not easy to control. It is easy to push the ring electrode into the uterine wall and cause damage and even cause perforation. In view of the difficulty of this method, when there are more tissues to be removed and the distant boundary cannot be seen clearly; when the lower boundary of the tissue to be removed is floating and it is difficult to perform antegrade resection; or when there are some wounds on the wound after antegrade resection. The residual tissue is connected to the wound surface and flutters. If it is difficult to perform anterograde resection, it should be performed by an experienced doctor.
The specific operation method is:
(1) First, place the hysteroscope on the surface of the tissue to be cut to expose the surgical field.
(2) Push the ring electrode out of the sheath and place it on the surface of the proximal end of the tissue to be cut.
(3) Step on the electric resection pedal to energize, push the ring electrode forward to cut into the tissue to an appropriate depth, push it backwards for a short distance, and cut it off when it reaches the distal edge of the tissue to be removed.
Transverse resection
Hysteroscopic high-frequency electric transverse resection is to cut the ring electrode from left to right, or from right to left. During the resection, the movement of the electric resection ring is mainly based on the appropriate lateral movement of the sheath. This method is suitable for removing the tissue at the bottom of the uterus and the uterine septum.
Vertical excision
The high-frequency electric vertical resection method of hysteroscope is to cut the ring electrode vertically from top to bottom. When cutting, the movement of the electric resection ring is small, and the main purpose of the hysteroscope sheath is to move up and down properly. This method is suitable for the removal of larger fibroids.
Previous
【Hysteroscopy】Endometrial Polyps
- Recommended news
- 【General Surgery Laparoscopy】Cholecystectomy
- Surgery Steps of Hysteroscopy for Intrauterine Adhesion
- [Percutaneous Endoscopic Lumbar Discectomy] Percutaneous endoscopic lumbar discectomy for lumbar disc herniation
- [Urology Cystoscopy Section] Cystoscopic Laser Lithotripsy
- [Laparoscopic Urology] Laparoscopic Radical Right Nephrectomy